Magnetic resonance imaging (MRI) is the gold standard of imaging diagnostics in many medical fields. But it is still far from always being readily available – even where it would be the best option. Technological progress is rapid. The next generation MRI could look very different.
Illustration: David Hänggi
A child of the 1970s, MRI is possibly the most
powerful diagnostic modality that healthcare ever invented. The first MRI image
of a human being was taken in 1977. With the 50th anniversary of this event
approaching, it is high time to ask how the technology has evolved – and
whether another transformation period is in store.
MRI today: The soft tissue giant
MRI today is largely about depicting water molecules, or protons, and soft tissue imaging has always been the hallmark of the technology. MRI is a champion of brain diagnostics. It not only visualizes tumors, ischemic strokes and bleedings, it also provides functional information, for example, by showing which areas of the brain are active in different situations.
Lower down the body, abdominal and pelvic imaging is another area in which MRI has outpaced other technologies in many diagnostic situations. While most pathologies can be seen in both CT and MRI scans, MRI is usually superior when it comes to detailed characterization of pathological lesions.
This is why gastroenterologists, oncologist and urologists who want to know what is happening in the liver, spleen, or prostate gland often choose an MRI over a CT scan.

Key investigation areas for MRI are soft tissue areas like brain, abdomen, vessels, ligaments, cartilages or muscles.
Fig.1: Courtesy of Tongji Hospital, Wuhan, China


Another key area for MRI is the heart and blood vessels. In cardiac MRI, the anatomy of ventricular walls and the cardiac valves can be depicted over time and supplemented with perfusion data and tissue characteristics. MRI can be used as a one-stop-shop for diagnosing cardiac conditions of all kinds, and for measuring myocardial and valve function in great detail.
Finally, MRI is the gold standard when it comes to questions relating to soft tissue pathologies in the musculoskeletal system, be it ligaments, cartilages or muscles. And, since MRI is a technology that requires neither radiation nor radioactive tracers, it is the diagnostic method of choice in children in just about any case except bone fractures.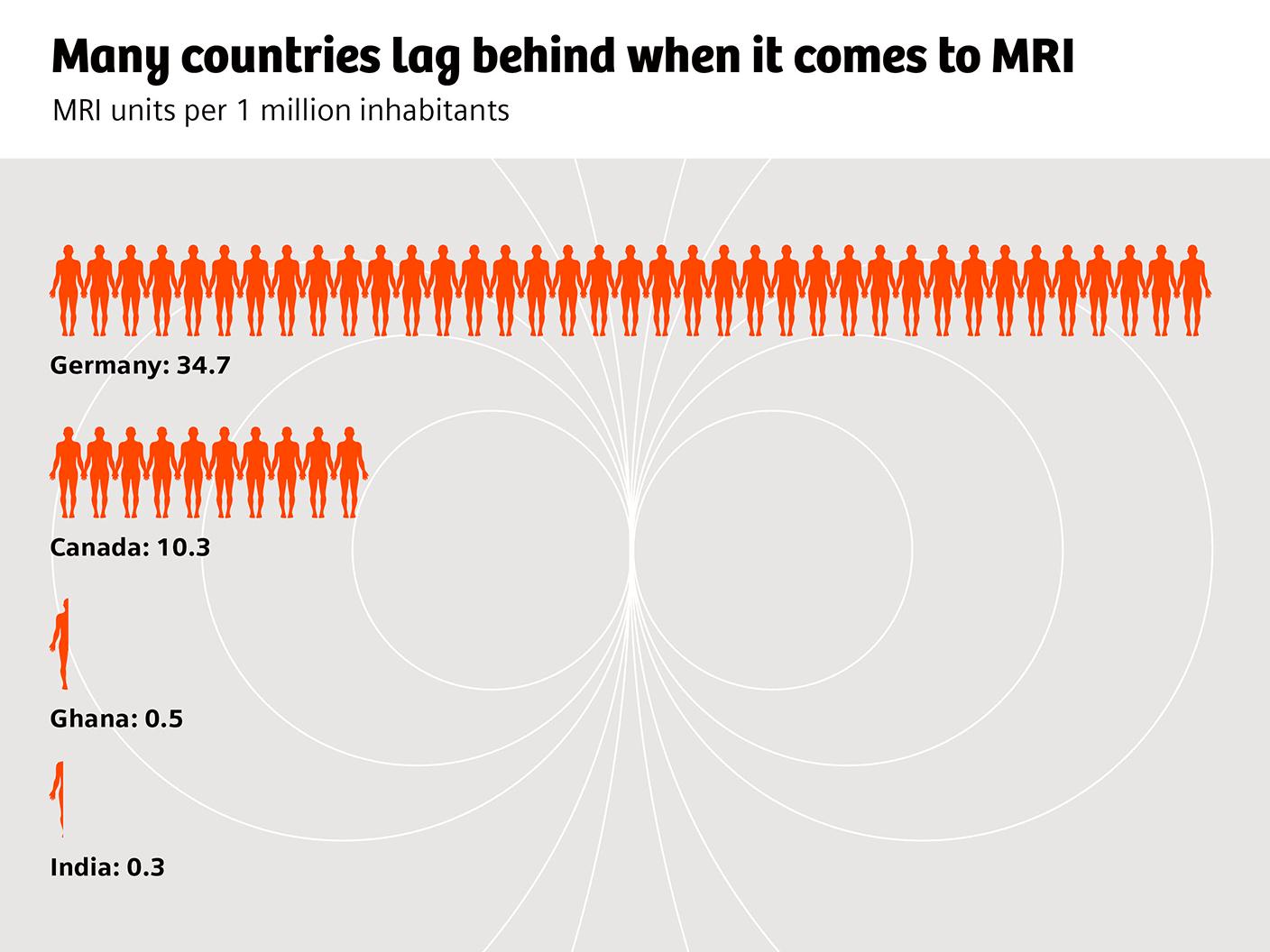
The challenge of accessibility
Despite its strengths, MRI is far from being universally accessible. In the OECD countries, for example, on average more than twice as many CT examinations as MRI scans are performed per 1000 inhabitants. Waiting times for an MRI scan are usually much longer than for a CT. There are also huge geographic variations: in Germany and Austria, the annual number of MRI examinations is bigger than the number of CT scans. In most other OECD countries, it is the other way round, and in less developed countries, the density of MRI scanning units is generally very low.
Why is that? The short answer would be that MRI is complex and expensive. But let us take a closer look. MRI machines require a superconducting magnet and thus considerable cooling, usually achieved by utilizing hundreds of liters of liquid helium coolant. This magnet technology explains why MRI machines are typically complex to site. In the case of an emergency or unplanned system quench, superconductivity is stopped, and the liquid helium boils off and expands exiting through a quench pipe to the atmosphere. This quench pipe is essential and is often costly and expensive to install because it demands building modifications. MRI’s are also heavy and along with all their associated control equipment typically require a large amount of space.
In other words, accessibility to MRI is not only limited because of the scanner costs. There are also many infrastructural requirements that can be difficult or expensive to fulfill. And – think of helium refills and downtimes – MRI service, too, is more demanding and thus more costly. It is not by chance that, in many countries, MRI imaging tends to be much more centralized than CT imaging. A modern CT scanner can be placed almost anywhere: on the 20th floor, in a small operating theater, in an ER room, or on a critical care ward. With a conventional MRI system, this can be very difficult or even impossible to do.


Some patients are too obese for MRI examinations, some patients have to be excluded if they suffer from claustrophobia.
Other challenges
Complexity and lack of usability are adding to accessibility issues. The physics behind MRI is complex. For any given organ in the body, there are a number of ways to look at it, a number of “MR sequences” that can be chosen. Each one may be “correct”, depending on what exactly it is that the radiologist is looking for. Seen this way, taking an MRI picture is like photography in the old days, when it was mechanical. It is a fascinating technology, but it requires a certain dedication and expertise.
Artifacts are another challenge. Small changes in the settings can result in disturbing artifacts, and it requires a certain expertise to mitigate them. Even patients themselves can be the source of artifacts, for example when they carry an implant. To get an image of sufficient quality can be time-consuming in implant patients. Some implants on the market are fully incompatible with MRI. Patients with these implants have to be excluded from scanning in conventional scanners.
There are other patients that are completely unsuitable for MRI: some are simply too obese, a problem that could be addressed by enlarging the bore. The stronger the magnetic field, the more complex and costly it becomes to produce MRI units with large patient bores. Even slimmer patients might have to be excluded if they suffer from claustrophobia, which can be caused by the small bore-size and the noise that conventional MRI machines produce.All in all, performing an MRI examination takes longer, and can be trickier than performing a CT examination. As a consequence, delegating an MRI examination to a technical assistant is less straight-forward than delegating a CT examination. Hub-and-spoke scenarios, increasingly common in CT imaging, are rare in MRI.
The transforming power of innovation
Medical technology has made considerable progress in recent years, the big trends being miniaturization, digitization, and automation. Given that MRI scanners are masterpieces of technology, how technological progress will affect them is a very legitimate question. There is reason to believe that the MRI landscape might evolve considerably, or even change forever.
What, for example, if technological innovations became possible that allow for a much more efficient cooling? MRI machines would become less heavy, they would need less space, and building infrastructure requirements would diminish.
What if digitization and artificial intelligence led to a more standardized, less error-prone handling? What if patients could be placed in the scanners faster, sequences were chosen more or less automatically, and artifacts were detected and resolved by software? We already know the answer: both patient preparation time and imaging acquisition time would reduce further, and technical assistants would have much less difficulty in performing routine examinations.
What, finally, if fewer patients had to be excluded from an MRI because bores are wider and machines are quieter and less frightening? What if a scanning platform was used that resulted in fewer artifacts? New clinical applications could become possible, and more patients overall could be diagnosed with MRI.Enter the future of MRI diagnostics
What is the long-term perspective? Healthcare systems around the world might rethink the way they organize imaging. MRI systems that are less costly, smaller, easier to use, and less error-prone could be deployed much more widely. Small hospitals, outpatient clinics of all kinds, and orthopedic practices, for example, could find it beneficial to have an MRI unit on site, either run by themselves or – following a hub-and-spoke-model – in cooperation with a radiological service provider. In such a scenario, radiologists would only provide the reports. In situations that require their expertise, they could also act as an active consultant, tele-operating the system if necessary.
For larger hospitals, smaller, more mobile, and less powerful MRI scanners could also hold an appeal. They could be used as overflow capacity – think of COVID-19 – but would also allow completely new types of services, for example providing MRI examinations in the emergency room, during interventions or on the ICU. An MRI platform that is less prone to artifacts could also open avenues towards new types of clinical applications, for example improved implant imaging or new possibilities for lung imaging.
Would there be a price to pay for MRI going this way? If we talk about smaller MRI platforms with less powerful magnets, it is inevitable that available signal-to-noise ratio would go down. However, rapid progress in digital post-processing technologies could to a large extend compensate for that. Furthermore, the new MRI machines would not replace high-end imaging. They would allow for new clinical scenarios. And they would make MRI available in the many, many places around the world it has been unable to reach for the past 40 years.About the Author
Philipp Grätzel von Grätz lives and works as a freelance medical journalist in Berlin. His specialties are digitalization, technology, and cardiovascular therapy.