By Mario Jreige, MD; Patrick Omoumi, MD; John O. Prior, MD, PhD; and Marie Nicod Lalonde, MD
Data courtesy of Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland


History
A 58-year-old patient with prostatic hypertrophy underwent a prostatectomy, which led to an incidental discovery of adenocarcinoma of the prostate that was staged at T2c N0 M0 with a Gleason score of 7 = 3 + 4.
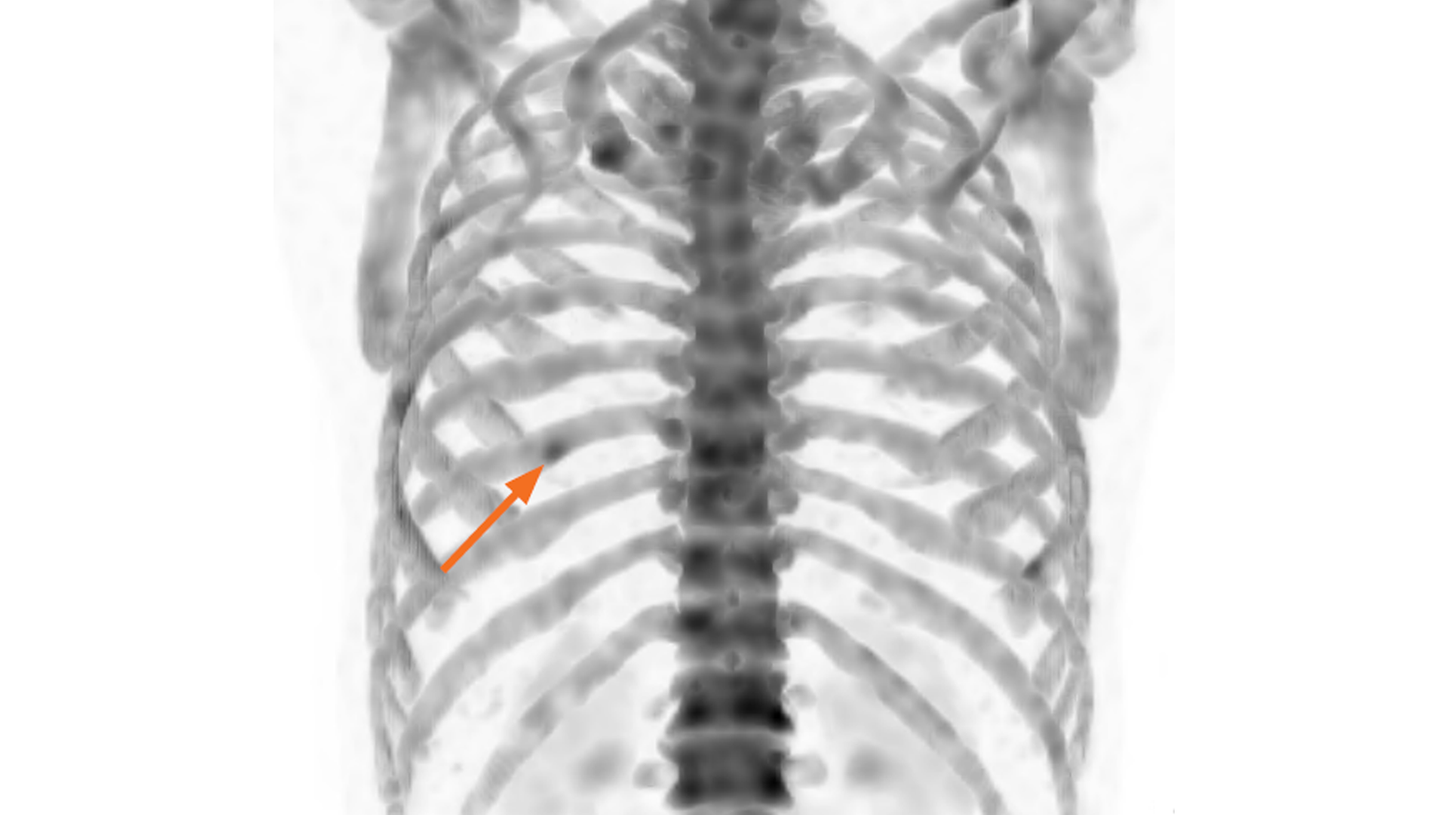
As part of the initial staging, a 99mTc DPD bone scan was performed on a Symbia Intevo™ 16 SPECT/CT. Three hours following intravenous (IV) administration of 18.9 mCi (700 MBq) of 99mTc DPD, initial planar acquisitions were conducted in the anterior and posterior views. A subsequent SPECT/CT examination using xSPECT Bone™ and xSPECT Quant™ was administered for the thorax.
Although the low intensity of uptake and the solitary nature of the rib lesion is suggestive of a benign origin, the patient’s history of prostate cancer was cause for suspicion. The SPECT/CT and xSPECT Quant findings were reviewed for better characterization of the rib lesion.

Findings
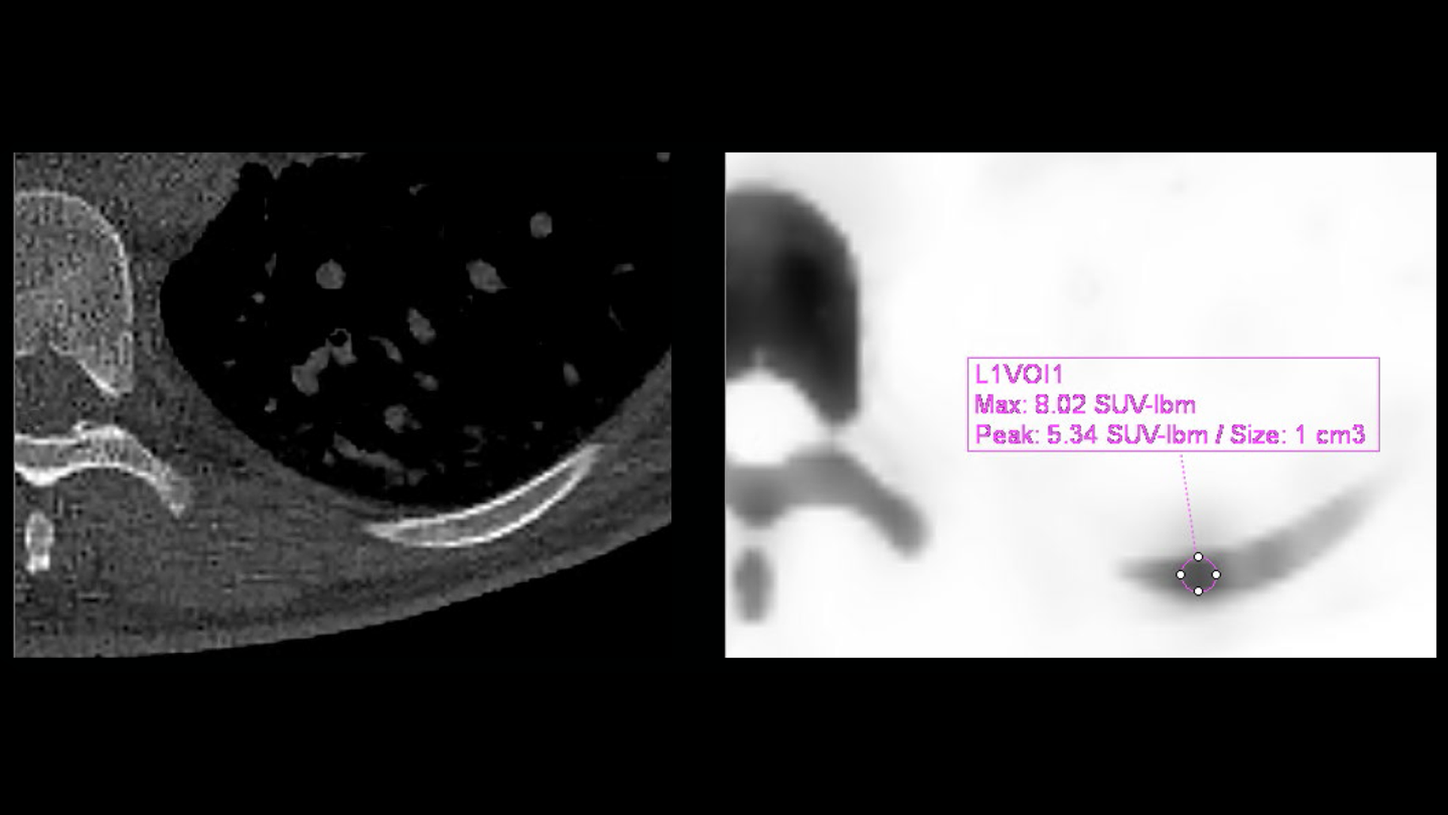
Quantitative SPECT/CT (Figure 4) demonstrated focal uptake in the left ninth rib, with a SUVmax of 8.02 mg/ml. The results correspond to an intramedullary lesion, without a sign of aggressive growth seen on CT (no cortical rupture or periosteal apposition), most likely of cartilaginous origin.
CT findings of an intramedullary lesion—without cortical erosion or periosteal reaction and thickening—along with the relatively low uptake of 99mTc DPD and low SUV observed on xSPECT Quant (< 20 mg/ml),1 were suggestive of a benign origin, most likely an enchondroma. Other possibilities included bone dysplasia or the sequelae of a previous bone infarction. Post-operative follow-up showed a non-detectable serum level of prostate-specific antigen (PSA) (< 0.03 ng/ml). The patient maintains a non-detectable PSA level from date to 16 months after surgery (latest follow-up date).


Comments
Solitary rib lesions seen in bone scintigraphy are commonly secondary to trauma or benign pathology, even in patients with known malignancy. However, the intensity of uptake and CT findings within the lesion are vital to the accurate characterization of such lesions. In this patient, the focal lesion in the left ninth rib showed low intensity of uptake and a low SUVmax of 8.02 with CT findings of a well-circumscribed intramedullary rib lesion without bony expansion, cortical erosion, or periosteal thickening. CT findings—along with low uptake intensity and low SUVmax related to a relatively minor level of skeletal hypermetabolism— were all suggestive of a benign origin of the rib lesion, which was deemed an enchondroma. The patient continues to maintain an undetectable level of serum PSA, thus confirming the absence of functioning metastases. xSPECT Quant enabled the estimation of lesion SUVmax, which was significantly below the usual levels seen in malignant lesions, thus supporting the diagnosis of a benign enchondroma.1


Conclusion
Low SUVmax in a suspicious focal rib lesion, obtained from xSPECT Quant in combination with CT information, helped in the diagnosis of a benign enchondroma in a patient with known prostate cancer.