By Iain Duncan, MD
Data courtesy of Garran Medical Imaging, Canberra, Australia

History
A 60-year-old woman with a history of anterior fixation and fusion of the C5-C6 vertebrae presented with chronic, dull neck pain. Cervical facet arthropathy was initially suspected to be the cause of the pain. The patient underwent a bone SPECT/CT scan using xSPECT Bone™.
The study was performed on a Symbia Intevo™ 2 system 3 hours following an intravenous injection of 23 mCi (850 MBq) of 99mTc-hydroxydiphosphonate (HDP). A diagnostic CT scan (110 kV, 49 eff mAs, 2 x 1.5 mm collimation) was followed by a SPECT acquisition (30 stops per detector, 18seconds per stop). xSPECT Bone reconstruction was performed using CT-based zone maps. Reconstructed xSPECT Bone data was subsequently fused with the CT for final interpretation. Standard 3DOSEM reconstruction was also performed and compared with the xSPECT Bone data. Quantitative estimation of tracer uptake from xSPECT Bone and xSPECT Quant™ acquisitions enabled determination of SUV within lesions and normal bone.

Findings
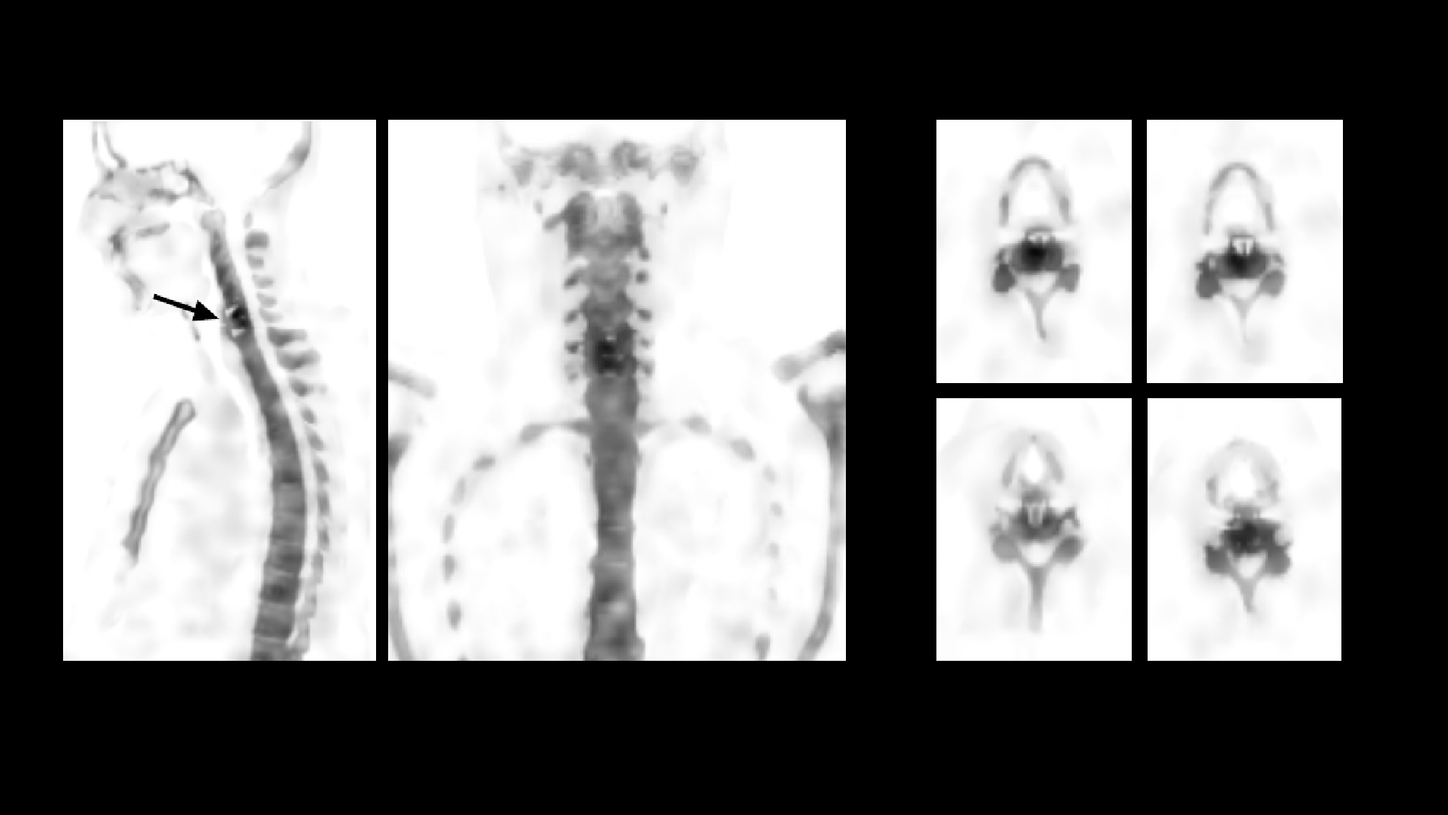
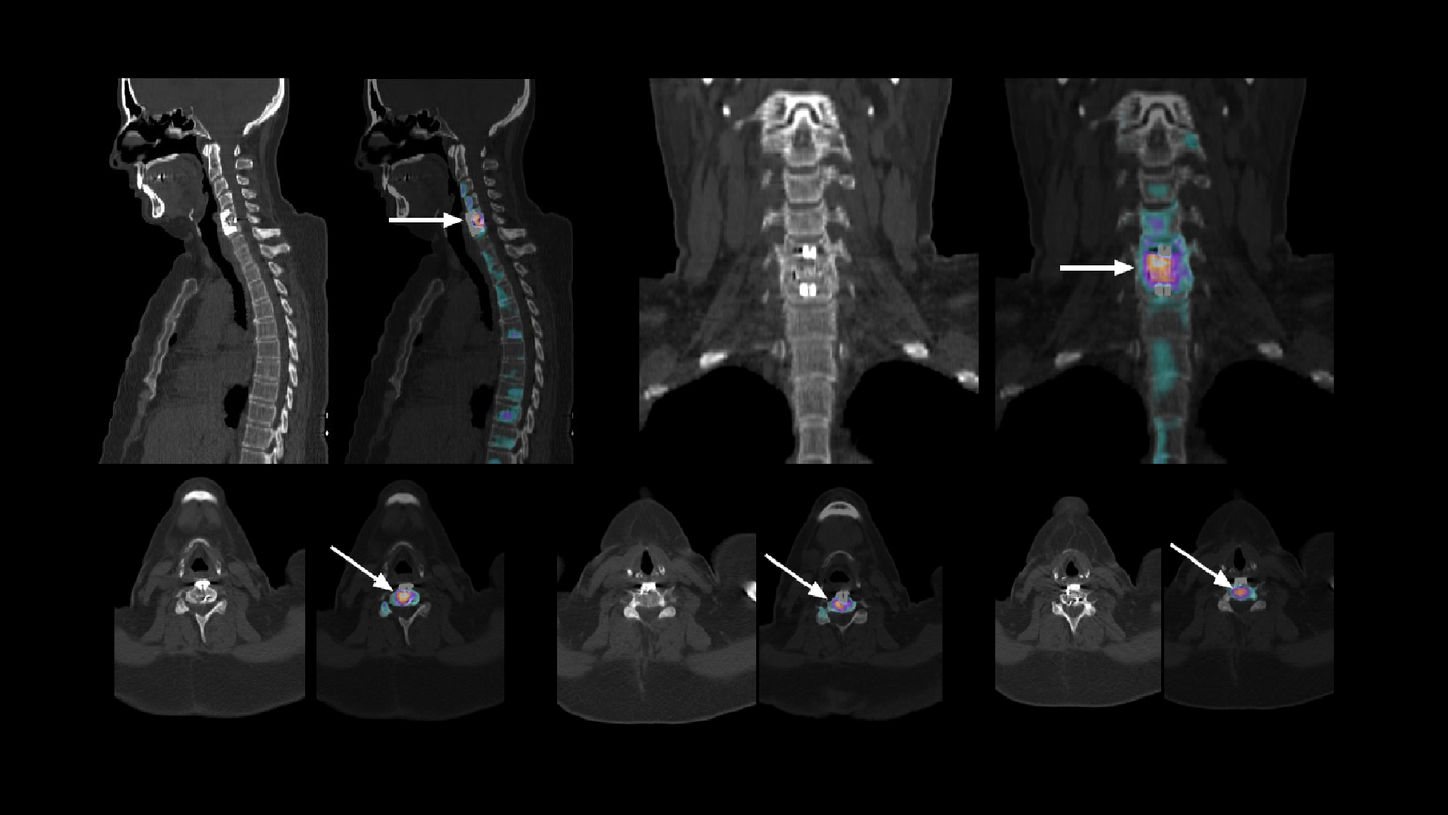
The CT, xSPECT Bone, and fused images in Figures 1-4 indicate there is focal hypermetabolism in C5-C6 disc space and adjacent vertebral end plates, which is consistent with bone stress, despite anterior fixation. The intensity of uptake and the significantly increased SUV (Figure 1) compared to normal cervical bone reflect avid bone stress, which is excessive considering the fusion was performed 2 years prior. Such excessive bone stress 2 years following anterior fixation with the highest focal hypermetabolism ( just adjacent to the upper fixation screw) appears to be related to possibility of failure of fusion with loosening of the upper fixation screw. The severe facet arthropathy of the right C5-C6 facet joint is secondary to shear stress caused by loosening of a fixation screw.


In the present study, xSPECT Bone was instrumental in the accurate localization of the focal hypermetabolism within the vertebral disc space close to the upper cervical fixation screw, which suggests that it may be the site of loosening with possible failure of fusion and secondary cervical facet arthropathy. A comparison of xSPECT Bone and standard 3DOSEM reconstructions clearly demonstrate the visual improvement in delineation of prosthetic margins, vertebral hypermetabolic foci, and vertebral body and facet edge definition, which significantly improve the visual localization of the pathology. The use of SUV in the hypermetabolic foci and comparison to normal vertebral SUV is a new benchmark enabled by xSPECT Quant™ to determine the degree of hypermetabolism related to shear stress and act as a baseline for subsequent post-therapy comparisons.

Comments
Anterior interbody fusion of the cervical vertebrae is a common treatment for cervical disc herniation or instability secondary to trauma. A discectomy is performed followed by the interbody fusion, which usually involves a bone graft placed between 2 vertebrae to replace the removed disc along with insertion of fixation screws above and below the bone graft with anterior plate fixation of the upper and lower cervical vertebral screws. A successful fixation usually leads to incorporation of the bone graft with the adjacent vertebral end plates creating a solid piece of bone out of the 2 vertebrae. The aim of the fixation screws and the anterior plate to hold them together is to create a rigid structure involving the adjacent vertebrae and bone graft in order to avoid motion between the vertebrae. Common complications following anterior cervical spine fixation include loosening of fixation screws, which may create shear stress and motion at the level of bone graft within the disc space, which may delay fusion or lead to failure of fusion. Additional complications include fracture of spinal screws as well as implant migration and psuedoarthrosis secondary to failure of fusion.


99mTc-MDP bone SPECT scans accurately reflect focal hypermetabolism within the cervical vertebral bodies, disc space, and facet joints and pedicles, which are secondary to shear stress caused by screw loosening, vertebral body instability, implant fracture, or failure of fusion. SPECT/CT is useful in exact localization of the focal hypermetabolism in relation to bone and prosthesis, which further improves interpretation of the pattern of hypermetabolism and helps define its cause. Bone SPECT/CT has been shown to be very sensitive in localizing sites of facet arthropathy that cause neck pain.1
Conclusion
xSPECT Bone sharply defined focal hypermetabolism in C5-C6 disc space adjacent to the upper cervical fixation screw, thereby suggesting failure of fusion due to loosening of the upper fixation screw with secondary cervical facet arthropathy.